Malignancy-associated Acanthosis Nigricans
Rather than commit a long list of unusual skin findings to memory, I'm going to try to get you to think more in terms of the Zen of the problem. When you see a particular presentation of, say, acanthosis nigricans, try to put it in a context. Is it new in onset? Does the patient have other predisposing issues such as obesity or metabolic syndrome that would explain it? Is it really dramatic, or less so? Acanthosis nigricans is a dime-a-dozen condition, but it it is particularly severe, in association with weight loss, or other constitutional symptoms such as night sweats or weakness, you might have a true-blue case of malignancy associated acanthosis nigricans. Look for adenocarcinomas, in that is the usual combination.
I am going to list a few of the signs of internal malignancy, but this list is neither all-inclusive nor will I attempt to describe them.
Leser-Trelat (sudden appearance of itchy SKs)
Bazex Syndrome (acrokeratosis paraneoplastica)
Trousseau's Sign (migratory thrombophlebitis)
Erythema Gyratum Repens
Necrolytic Migratory Erythema
Hypertrichosis lanuginosa
Paraneoplastic pemphigus
Flushing (associated with carcinoid)
Sweet's Syndrome (Leukemia)
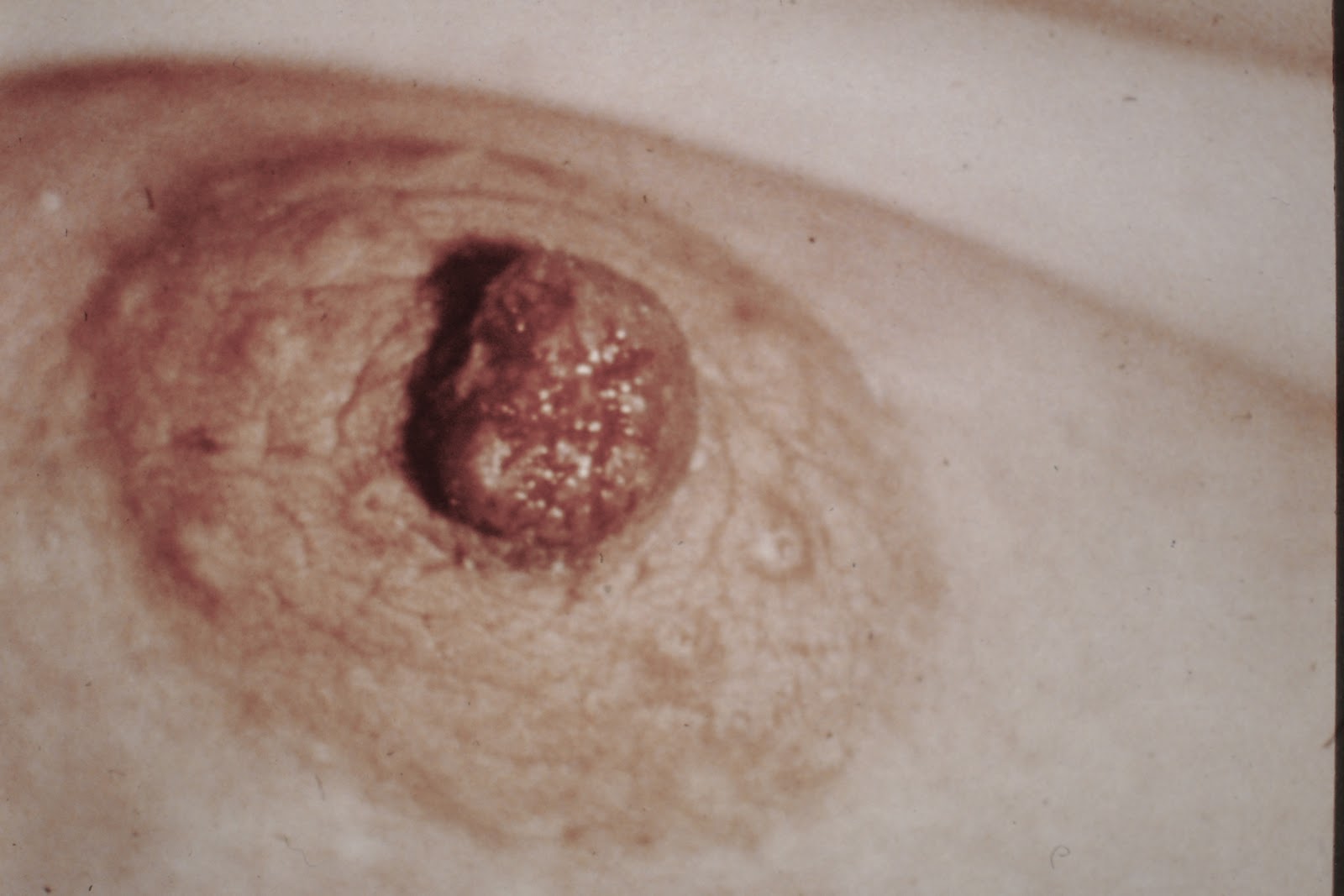
Paget's Disease of the Breast
Extramammary Paget's
Dermatomyositis
Acquired Ichthyosis
Tripe Palms
Sister Mary Joseph's nodule (For a bonus point, who was Sister Mary Joseph?)
Once again, these are not the only ones out there, but if you know these disease presentations, you will often be the smartest one in the room, if not the entire building. And that's a good thing...